what are the following answers regarding the screenshot article.
1. Identify the independent variable.
2. What is the level of measurement of the independent variable?
3. Identify the dependent variable.
4. What is the level of measurement of the dependent variable?
5. What is the total sample size (n)?
6. What measurement tools did the researchers use to collect data?
7. Did the researchers report validity and reliability statistics for the measurement tools?
8.If so, what statistical test was reported? What were the results of the statistical test? What do these results indicate?
1. Why did the researchers perform a power analysis prior to conducting the study? What were the results of the power analysis?
2. What was one major limitation of this study? Which type error (Type I or Type II) is most likely to occur in this study? Define this error. How can the researchers decrease the risk of this type error?
3. What is your impression of the study results? Would this study prompt you to make a change in clinical practice?
4. What is something you learned, understand better, or still do not understand?
Image transcription text
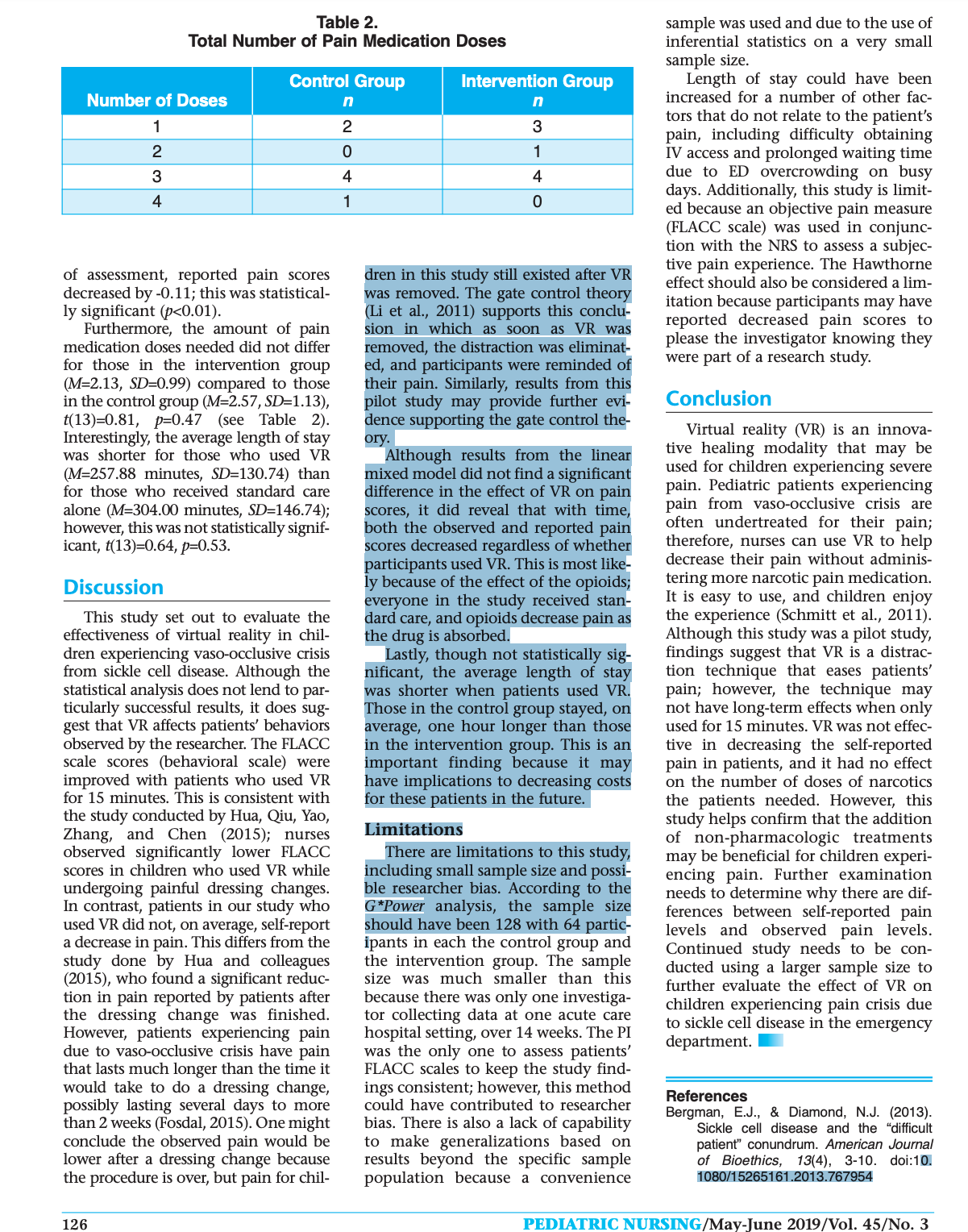
Table 2. Total Number of Pain Medication Doses sample was used and due to the use of inferential statistics on a very small sample size. Control Group Intervention Group Length of stay could have been Number of Doses n n increased for a number of other fac- 1 2 3 tors that do not relate to the patient’s 0 pain, including difficulty obtaining IV access and prolonged waiting time 4 due to ED overcrowding on busy 1 A – 0 days. Additionally, this study is limit- ed because an objective pain measure (FLACC scale) was used in conjunc tion with the NRS to assess a subject of assessment, reported pain scores dren in this study still existed after VR tive pain experience. The Hawthorne decreased by -0.11; this was statistical- was removed. The gate control theory effect should also be considered a lim- y significant (p<0.01). (Li et al., 2011) supports this conclu itation because participants may have Furthermore, the amount of pain sion in which as soon as VR was reported decreased pain scores to medication doses needed did not differ removed, the distraction was eliminat please the investigator knowing they for those in the intervention group ed, and participants were reminded of were part of a research study. (M=2.13, SD=0.99) compared to those in the control group (M=2.57, SD=1.13), their pain. Similarly, results from this t(13)=0.81, p=0.47 (see Table 2). pilot study may provide further evi- Conclusion dence supporting the gate control the- Interestingly, the average length of stay ory. Virtual reality (VR) is an innova- was shorter for those who used VR Although results from the linear tive healing modality that may be (M=257.88 minutes, SD=130.74) than mixed model did not find a significant used for children experiencing severe for those who received standard care difference in the effect of VR on pain pain. Pediatric patients experiencing alone (M=304.00 minutes, SD=146.74); scores, it did reveal that with time, pain from vaso-occlusive crisis are however, this was not statistically signif both the observed and reported pain often undertreated for their pain; icant, t(13)=0.64, p=0.53. scores decreased regardless of whether therefore, nurses can use VR to help participants used VR. This is most like- decrease their pain without adminis- Discussion ly because of the effect of the opioids; tering more narcotic pain medication. This study set out to evaluate the everyone in the study received stan- It is easy to use, and children enjoy dard care, and opioids decrease pain as the experience (Schmitt et al., 2011). effectiveness of virtual reality in chil- the drug is absorbed. Although this study was a pilot study, dren experiencing vaso-occlusive crisis from sickle cell disease. Although the Lastly, though not statistically sig- findings suggest that VR is a distrac nificant, the average length of stay tion technique that eases patients’ statistical analysis does not lend to par- ticularly successful results, it does sug- was shorter when patients used VR. Those in the control group stayed, on pain; however, the technique may not have long-term effects when only gest that VR affects patients’ behaviors observed by the researcher. The FLACC average, one hour longer than those used for 15 minutes. VR was not effect live in decreasing the self-reported scale scores (behavioral scale) were n the intervention group. This is an improved with patients who used VR important finding because it may pain in patients, and it had no effect for 15 minutes. This is consistent with have implications to decreasing costs on the number of doses of narcotics the study conducted by Hua, Qiu, Yao, for these patients in the future. the patients needed. However, this Zhang, and Chen (2015); nurses Limitations study helps confirm that the addition observed significantly lower FLACC There are limitations to this study, of non-pharmacologic treatments scores in children who used VR while including small sample size and possi- may be beneficial for children experi- undergoing painful dressing changes. ble researcher bias. According to the encing pain. Further examination In contrast, patients in our study who G*Power analysis, the sample size needs to determine why there are dif- used VR did not, on average, self-report should have been 128 with 64 partic- ferences between self-reported pain a decrease in pain. This differs from the ipants in each the control group and levels and observed pain levels. study done by Hua and colleagues the intervention group. The sample Continued study needs to be con- (2015), who found a significant reduc- size was much smaller than this ducted using a larger sample size to tion in pain reported by patients after because there was only one investiga- further evaluate the effect of VR on the dressing change was finished. tor collecting data at one acute care children experiencing pain crisis due However, patients experiencing pain hospital setting, over 14 weeks. The PI to sickle cell disease in the emergency due to vaso-occlusive crisis have pain was the only one to assess patients’ department. that lasts much longer than the time it FLACC scales to keep the study find- would take to do a dressing change, ings consistent; however, this method possibly lasting several days to more References than 2 weeks (Fosdal, 2015). One might could have contributed to researcher Bergman, E.J., & Diamond, N.J. (2013). conclude the observed pain would be bias. There is also a lack of capability to make generalizations based on Sickle cell disease and the "difficult lower after a dressing change because results beyond the specific sample patient" conundrum. American Journal of Bioethics, 13(4), 3-10. doi:10. the procedure is over, but pain for chil- population because a convenience 1080/15265161.2013.767954 126 ATRIC NURSING/May-June 2019/Vol. 45/No. 3
Image transcription text
nistration, included both the NRS Table 1. score reported by the patient and the Participant Demographics FLACC pain score observed by the PI. The PI documented the pain level Variable % reported and observed at the start of n the study, the pain level observed at Gender the 5-minute time interval, and the Male 40.0 pain level reported and observed 15 minutes after the initial pain medica- Female 9 60.0 tion with the respective times in an Ethnicity Excel spreadsheet. The changes in 15 100.0 scores between the different assess- African American ment time intervals were calculated. Age (years) The PI also recorded how many doses 8 to 10 3 19.9 of pain medication the patient requested and the total length of stay 11 to 13 33.3 in the ED. All data collected corre- 14 to 17 7 46.5 sponded to a coded number to repre- sent each participant without using private identification information. Figure 1. The PI obtained data for all patients, Average FLACC Pain Level Changes including the observed and reported pain levels, to keep the data collection consistent and accurate. 7 Statistical Analysis 6 Results collected in this research project were analyzed using an inde- pendent samples t test to compare the pain levels at all time intervals for par- ticipants in the intervention and con- trol groups. Additionally, a linear mixed model in R was used to test N W A effects of the intervention in relation to time. Confidence interval was 95%, Pain Level (FLACC Scale) – and all p-levels were considered signif- icant at the level of 0.05. O 0 5 15 Results Time (Minutes) Fifteen children with vaso-occlu- -Standard sive crisis participated in the study. -VR Their ages ranged from 8 to 17 years. The median age of participants was 13 years. Sixty percent of participants were female, and 40% were male. All participants were African American for 15 minutes (M=5.71, SD=2.75) or t(13)=-1.09, p=0.30, but this difference (see Table 1). The average observed received standard care alone (M=5.25, SD=2.25), t(13)=-0.36, p=0.73. The was not statistically significant. The linear mixed model found the pain scores using the FLACC scale average pain level reported by patients effect of the intervention reduced were significantly lower for patients using VR for 5 minutes (M=1.57, was actually higher in those who used VR. Those who used VR had a greater FLACC score by -1.65; although, this SD=1.51, n=7) than the average pain was not statistically significant scores documented for participants in decrease in observed pain from the ini- p=0.11). However, for every minute the control group (M=4.25, SD=2.12, tial assessment compared to the score n=8), t(13)=2.78, p=0.01 (see Figure 1). observed 5 minutes later (M=3.29, increase from the initial measure- ment, FLACC scores were reduced by -0.18, which is statistically significant The average observed pain level using SD=1.38). However, there was no sig- the FLACC scale was lower at 15 min- nificant change in the pain observed p<0.01). This model was also used to utes in those who used VR (M=1.29, when compared to those in the con- assess the effect of the intervention SD=1.70); however, scores did not dif- trol group (M=1.75, SD=2.05), t(13)=- 1.67, p=0.11. Further, there was a on reported pain scores, and the effect fer significantly from those who did of VR did not reduce reported pain not use VR (M=3.25, SD=2.12), greater decrease in pain observed from scores on average. In fact, there was t(13)=1.96, p=0.07. the time of the initial assessment to the one 15 minutes later for those who an increase in reported pain scores by Self-reported pain scores using the 0.13, though this was not statistically NRS did not significantly differ on experienced VR (M=3.57, SD=0.53) significant (p=0.90). Similar to the average whether the patients used VR when compared to those who received standard care only (M=2.75, SD=2.05), effect on FLACC scores, as every minute passed during the 15 minutes
Image transcription text
arched, rigid, or jerking; is crying steadily, screaming, or sobbing with tients and their parents/legal guar- dians. Participants were made aware utes after the IV opioid was adminis- tered. frequent complaints; and is difficult to that participation was voluntary and Participants in the intervention console or comfort. This pain assess- ment tool is typically recommended that they could discontinue their par- group were given their first dose of IV pain medication and then used the VR for children aged 2 months to 7 years ticipation in the study at any point without penalty. Participants and par- (Srouji, Ratnapalan, & Schneeweiss, 2010); however, multiple researchers ents/legal guardians could ask ques- for 15 minutes. This amount of time was chosen because virtual reality has have evaluated and confirmed validity tions prior to the start of the study been successful in other studies and reliability of this scale in various and during the study, and all ques- tions were answered. No identifying Dascal et al., 2017; Gershon, Zimand, pediatric age groups when patients are unable to self-report pain (Blount & information was collected in the Pickering, Rothbaum, & Hodges, 2004; Hoffman et al., 2011, Schmitt et Loiselle, 2009; Nilsson, Finnstrom, & study to protect patients’ right to pri- al., 2011) when it was used for medical Kokinsky, 2008; Voepel-Lewis, Zanotti, vacy procedures, which typically lasted no Dammeyer, & Merkel, 2010). Addi- Intervention more than 15 minutes. Using the FLACC scale, the PI observed the tionally, researchers Voepel-Lewis and The Google Daydream VR was colleagues (2010) reported criterion used for patients who were in the patient’s movement, activity, and and construct validity of the FLACC intervention group for 15 minutes facial expressions while the patient was wearing the headset to determine scale, as well as interrater reliability, after they received their IV pain med- 0.882. and found the Cronbach alpha to be ication (standard care). The VR con- the level of pain 5 minutes into the sisted of a headset that wears like a experience; this is the time at which The NRS is used to assess pain by ask- IV morphine reaches its peak effect ing a patient to rate his/her pain on a pair of goggles and a screen from a Google Pixel cell phone inside the (Larijani, Goldberg, Warshal, & Gratz, scale of 0 to 10, with 0 representing no headset that illuminated in front of 2005). The FLACC scale was used at this point to enable the PI to assess the pain, and 10 representing the worst the patient’s eyes. While wearing the pain possible (Myrvik et al., 2013). Until headset, the patient could move patients’ pain rather than interrupting recently, there were limited data sup- his/her head around to see a full 360- the patients while using the VR to porting the use of the NRS in children (Castarlenas, Jensen, von Baeyer, & degree view of the image, which assess pain on a reported scale. immersed the patient into a virtual Interrupting the experience could Miro, 2017). Newer studies have evalu- remind patients of their pain and ated the psychometric properties of this world. Participants could choose from five different applications that were potentially alter the true effect of the pain scale, confirming its appropriate use for children in clinical practice. downloaded onto the Google Pixel VR. After 15 minutes of using VR, the cell phone. The choices of applica- PI assessed the patients’ level of pain Miro, Castarlenas, and Huguet (2009) tions included 1) Wonderglade, an by using the NRS and the FLACC scale found a strong association between the application with several interactive again. Both scales were used to assess NRS and Faces Pain Scale -Revised mini games, such as basketball and pain before and after the intervention, (Hicks, von Baeyer, Spafford, van so a comparison could be made Korlaar, & Goodenough, 2001, which golf; 2) Ocean Rift, where the partici- demonstrated convergent validity. The pant can explore the ocean and its between the reported pain by the patients and the observed pain level authors concluded that the NRS could inhabitants; 3) Karts Sprint, a car rac- be used to assess pain in children greater ing game; 4) Ace Fishing, a 3D fishing from the PI. Patients in the control group received standard care for sickle cell than age 8 years. Fernando, Rifaya, adventure; and 5) The Turning Forest, where a narrator reads a story while Asantha, Chandarathna, and Wijeratna the participant encounters a magical pain and their level of pain was (2017) compared the NRS with the forest. The headset blocked the view- assessed 5 minutes after they received Faces Pain Scale and the Verbal Pain er’s vision of his/her real surround- their first dose of IV pain medication Rating scale (von Baeyer, 2006) in chil- ings. The phone was set to Airplane also using the FLACC scale. The PI assessed pain 15 minutes after the dren aged 4 to 12 years and found inter- 0.902). nal consistency (Cronbach alpha = Mode so Wi-Fi and cellular data were not used at the time the video was dis- first narcotic medication was adminis- tered using the NRS and the FLACC played. scale again. The difference in pain Ethical Considerations Data Collection level from the time of initial medica- The Institutional Review Board The principal investigator (PI) tion administration and 15 minutes approved this study prior to data col- (SDH) collected data at one acute care later was compared. The FLACC scale lection. Informed consent was hospital ED setting, over 14 weeks. All was used to assess pain 5 minutes obtained from parents/legal guar- patients used the NRS to self-report after the narcotic was given, so it dians of participants, and assent was their pain levels at two points in time: could be compared to the pain level obtained from all participants. Mini- mal risks were involved with the once prior to the IV opioid adminis- observed in patients in the interven- tration (standard care) and then again tion group with the same scale. 15 minutes post-medication adminis- In sum, for both groups, the initial study, and participants were made aware of risks prior to participating. tration. At the same two points in assessment included the NRS reported Potential risks included nausea/ time, the PI also used the FLACC scale by the patient and the FLACC pain motion sickness related to the VR and to record observations of the patient’s score observed by the PI. Then the PI eyestrain. Benefits of reducing pain pain levels. For all patients, the PI also assessed pain using the FLACC scale 5 without using narcotic pain medica- conducted one more observational minutes after medication administra- tion was also explained to the pa- assessment, which occurred 5 min- tion. Lastly, the assessment at the 15- minute mark, post-medication admi-
Image transcription text
tient pain management, and on aver- found a 44%, 32%, and 27% reduc- age, this occurs with about 42% of tion respectively when VR was used method to evaluate the effective- these patients (Frei-Jones, Baxter, Rogers, & Buchanan, 2008). These fre- compared to when VR was not used. ness of VR as a non-pharmacolog There was a significant change in the ic therapy for children experience quent pain crises and hospital admis sions affect pediatric patients, their experienced pain level when virtual ing vaso-occlusive crisis in the ED. Miller, and Kimble (2012) assessed the Sample families, and their quality of life (Fisak, reality was used. Kipping, Rodger, Belkin, von Lehe, & Bansal, 2012). Two barriers to adequately manag- effectiveness of the use of VR for ado- A total of 15 pediatric patients lescent burn patients during dressing between the ages of 8 and 18 years ing sickle cell pain/vaso-occlusive crisis changes. with sickle cell crisis volunteered to in pediatric patients include the fre- Nurses and caregivers observed pain and patients’ self- participate in the study, which took quent necessity of several doses of nar- reported pain. There was a statistically place in a pediatric ED at an urban cotics and the discomfort level of ordering these medications among ED significant reduction in pain as teaching hospital in the Northeast. providers (Bergman & Diamond, observed by the nurses, and the length Systematic sampling was used in of time for the procedure was which every other patient was 2013). Porter, Feinglass, Artz, Hafner, decreased in patients who used VR assigned to the control group (those and Tanabe (2012) concluded that 53% of ED physicians believed approx- compared to those who received stan- who received standard care alone) or dard distraction. the intervention group (those who imately 20% of their patients with sickle cell disease were addicted to nar- In the adult literature, Hoffman, received standard care along with Chambers, Meyer, Arceneaux, and VR). Standard care at the acute care cotics, and 30% of ED nurses were hes- Russell (2011) completed a study to hospital consisted of IV narcotics itant to give these patients high doses of narcotics. Historically, ED nurses evaluate how VR affects pain levels in every 30 minutes as needed for up to patients with burns undergoing three doses. Patients were included in have tried adding non-pharmacologic therapies and distraction techniques to wound debridement in a hydrothera- the study if they presented to the ED help reduce pain without having to py tank. Hoffman and colleagues with vaso-occlusive crisis, were administer more medication (Dobson (2011) found that patients who had between the ages of 8 and 18 years, initially reported the most severe pain were English-speaking, and had a par- & Byrne, 2014). had a 41% reduction in pain level ent or legal guardian with them. while using VR. Although participants Patients were excluded from the study VR for Pain Control in this study were not children, results if they had used VR before, if they had Healthcare providers are typically presented with other conditions that interested in the use of non-pharma- support that even the most severe pain cologic interventions to augment pain can be reduced using VR. could be contributing to their pain, or The gate control theory helps if they had a history of seizures or in children because it is seen as an motion sickness because these were essential part of pain management explain how VR works to reduce pain. potential side effects of using VR. A (Wente, 2013). One innovative type of According to this theory, humans have limited capacity for attention. When G*Power analysis was conducted to non-pharmacologic tool is virtual real- ity (VR). VR is a computer hardware focused on a noxious stimulus, it is per- determine a desired sample size of ceived as painful. However, when 128, with 64 participants in each the and software device that creates simu- control group and the intervention lated environments to look and feel focused on a pleasant stimulus, the real (Yamato, Pompeu, Pompeu, & noxious stimulus is perceived as less group, using a standard power of 0.8, intense and severe (Li, Montano, Chen, along with an effect size of 0.5, and Hassett, 2016). VR is easily adminis- & Gold, 2011). The purpose of this an alpha set to 0.05. tered and can be used as a distraction study was to determine the effective- Instruments for children experiencing pain. Although empirical studies are sparse, ness of VR in reducing pain and the amount of pain medication needed in For all participants, pain levels evidence is building to support the use of VR to augment patients’ pain. pediatric patients with sickle cell were assessed using both a behavioral pain/vaso-occlusive crisis. Using the scale (FLACC scale) and a self-report Schmitt and colleagues (2011) con- scale (NRS). ducted a randomized, controlled gate control theory, this study aimed to The FLACC Behavioral Pain Assess- study using a crossover design to answer the following two research ment Scale includes an assessment of examine the effects of VR as an questions: 1. Do pain scores for pediatric sickle face, legs, activity, cry, and consolabili- adjunctive treatment for pediatric ty as five different components of pain burn patients undergoing range-of- cell patients who are experiencing pain crisis in the ED decrease with observed in a patient (Merkel, Voepel- motion exercises as part of physical the use of VR? Lewis, Shayevitz, & Malviya, 1997). therapy. The sample consisted of 54 2. Does a VR intervention for chil- Each of the five categories is scored on participants aged 6 to 19 years. dren with sickle cell crisis in the ED a scale of 0 to 2 based on the severity, Participants were medicated with with a total possible range of 0 to 10. A standard pre-procedure analgesia, and decrease the use of pain medica- tions? score of 0 indicates the patient has no everyone completed physical therapy particular facial expression or is smil- with an equal amount of time spent ing; has a normal position or is with and without using VR in the Methods relaxed; is lying quietly and moves eas- same session. Schmitt and colleagues ily; has no cry; and is content and (2011) assessed the cognitive, affect Design relaxed. A score of 10 indicates the tive, and sensory components of pain A quasi-experimental research patient has frequent to constant quiv- after each treatment condition and design was used as the research ering chin or clenched jaw; is kicking his/her legs or has them drawn up; is
Image transcription text
S ickle cell disease affects approx- imately 100,000 Americans, Diaz-Hennessey, S., O’Shea, E.R., & King, K. (2019). Virtual reality: Augmenting and according to global new- the acute pain experience in children. Pediatric Nursing, 45(3), 122-127. born estimates, approximately 300,000 infants are born with sickle The purpose of this pilot study was to determine the effect of virtual reality (VR) cell disease each year (Piel, Steinberg, & on acute pain in pediatric patients with sickle cell disease experiencing vaso- Rees, 2017). Vaso-occlusive crisis is a occlusive crisis in one acute-care pediatric emergency department (ED). The complication of the disease that causes randomized sample consisted of 15 participants aged 8 to 17 years admitted to severe pain. Children require prescrip the ED with vaso-occlusive crisis. The control group received standard ED treat- tions for pain medication, often opi- ment consisting of intravenous (IV) narcotics administered every 30 minutes as oids, during a vaso-occlusive crisis needed for up to 3 doses while the intervention group received VR for 15 minutes experienced at home, but they seek along with standard treatment. Pain was assessed using the Numerical Rating medical care in the emergency depart- Scale (NRS) and the Face, Legs, Activity, Cry, Consolability (FLACC) scale. Data ment (ED) when the pain is not were analyzed using an independent samples t test. Counter to hypotheses, improving. Fifty percent to 60% of vis- esults showed pain scores reported by patients using the NRS were not signifi- its to the ED among children with sick- cantly lower when using VR (M=5.71, SD=2.752) than for those who received le cell disease are due to pain (Meier & standard treatment. However, there was a statistically significant difference in the Miller, 2012). The following review of FLACC pain scores (behavioral scale) after 5 minutes of using the VR (p=0.01). the literature used the electronic data- Additionally, the average length of stay was shorter for the patients in the inter- bases CINAHL Plus, PubMed, and vention group. Although the self-reported pain scores by patients in this sample Cochrane Library. Key search terms did not vary significantly when using VR, there was a significant difference in the included virtual reality, sickle cell cri- observed pain scores. This pilot study’s data findings support the use of VR with sis, pain, children, and pediatrics. standard treatment in pediatric patients with sickle cell disease who present to the ED in vaso-occlusive crisis. Using multi-modal pain management strategies may decrease length of stay and improve pain scores. Sickle Cell Pain Control Methods Key Words: Virtual reality, sickle cell crisis, pain, children, pediatrics. An expert panel report released by the National Heart, Lung, and Blood Institute (NHLBI) (2014) included rec- and their effectiveness, and 3) admin- minophen, and ibuprofen were the ommendations for the management istering analgesic therapy within 30 most frequently administered medica- of pain in pediatric patients who pres- minutes of triage in the ED. The panel advised administering opioids accord- tions, which followed the hospital ent with vaso-occlusive crisis. The protocol. However, non-pharmacolog report emphasized the importance of ing to individualized pain protocols and reassessing pain every 15 to 30 ic interventions were not well docu- 1) assessing pain rapidly using self- mented and likely not used. Only 20% reported pain scales and observation, minutes. Although opioids and non- of reports mentioned using a hot pack 2) assessing previously used analgesics steroidal anti-inflammatory drugs and 37% of reports included distract NSAIDs) are typically used to manage tion by watching television. Pain vaso-occlusive crisis pain in the ED (Puri, Nottage, Hankins, & scores remained at a range from 4/10 to 10/10 using the Numerical Anghelescu, 2018), recommendations Rating Scale (NRS) and/or FLACC also include the use of non-pharma- scale throughout the hospital stay Samantha Diaz-Hennessey, DNP, FNP-BC, cologic modalities. is a Nurse Practitioner, Park Avenue Medical Despite the national guidelines, Vijenthira and colleagues (2012) con- Professionals, New York, NY. cluded that pain among this popula- children suffering from pain caused by tion should be addressed more aggres- Eileen R. O’Shea, DNP, APRN, PCNS-BC, vaso-occlusive crisis are still not sively and with more multimodal pain CHPPN, is a Professor, Egan School of achieving adequate pain relief management strategies as patients Nursing and Health Studies, Fairfield University, Fairfield, CT. (Vijenthira et al., 2012). Vijenthira continued to report pain even with and colleagues (2012) completed a medication management. Kyle King, is an Undergraduate Student, chart review of 50 pediatric patients When pain is not adequately con- Dolan Business School, Fairfield University, who were hospitalized for sickle cell trolled during an ED visit, patients with